- Share
- Share on Facebook
- Share on Twitter
- Share on LinkedIn
- Share url
Background
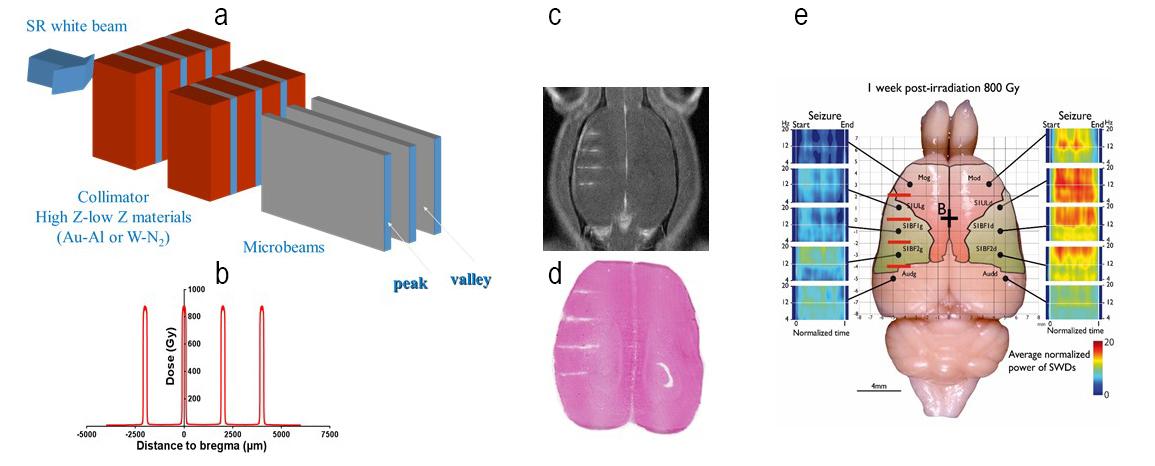
Other brain diseases involving specific brain areas could benefit from the knowledge and expertise gained during the development of MRT for brain tumours. Among these pathologies, some forms of epilepsies clearly appear as first choice candidates. Epilepsy is a devastating multi-causal chronic disease characterized by recurrent spontaneous seizures and affects about 1% of the population worldwide. Drug-resistant epilepsies, which account for about one third of adult epileptic patients, represent a socioeconomic burden at the individual, familial, societal and political levels in all countries across the globe. Some patients may benefit from resective surgery of the epileptogenic zone only when the epileptic zone is (i) focal, (ii) clearly identified and (iii) can be safely removed (1). Therefore, only a limited number of patients can benefit from such a surgical approach. Modern radiosurgical devices such as Gamma Knife® and Cyberknife® (2) have provided satisfying results in treating various types of epilepsies associated with arterio-venous malformations, cavernomas, tumours, mesio-temporal sclerosis and hypothalamic hamartomas (see: (3) for review). However, the reported failures in radiosurgical treatment of epileptic foci are often correlated with the radiosensitivity of normal tissues surrounding the lesion, which sets the limit to the radiation dose that can be safely delivered within the target (4). In this context, our collaboration with the group of Antoine Depaulis (Grenoble Institut of Neuroscience) has allowed to investigate during the last 5 years the use of MRT to suppress seizures in animal models. Our working hypothesis is based on several studies in patients (5) and animal models (6) suggesting that an antiepileptic effect could be obtained even if the irradiation did not result in necrosis of the targeted structure.
Using the Genetic Absence Epilepsy Rats from Strasbourg (GAERS) (7), a well-recognized and well described rat model for idiopathic generalized epilepsy in which seizures are initiated in the somato-sensory cortex, we have performed several sets of experiments showing the efficacy of MRT to suppress seizures for a duration of up to 5 months (8, 9). We further demonstrated at the cellular level that MRT reduces the possibility of ictogenic neurons to get synchronized (9).
Objectives
We will further explore the therapeutical value of MRT in treating drug-resistant epilepsies with a "tumour-like" focus. In this respect, focal epilepsies associated with (i) hippocampal sclerosis and (ii) cortical dysplasia appear as the first choice candidate to perform a proof of concept clinical trial in which the patient can be offered MRT followed by resective surgery in case of failure. To this aim we will apply protocols in two rat models of (i) mesiotemporal lobe epilepsy associated with hippocampal sclerosis following local application of kainate (10) and (ii) cortical dysplasia induced by a treatment with methylazoxymethanol during embryogenesis (11). In both models, as in our previous studies, seizures will be monitored by EEG and electrophysiological techniques. Tissular and behavioural consequences will be assessed by MRI, immunohistological labelling and different tests to detect possible motor or sensory impairments.
The possibility to induce cortical dysplasia in pigs by a treatment with methylazoxymethanol during embryogenesis will be explored to later explore the effects of MRT on the dysplasic area.
A PSS system was developed at the ESRF for the safe irradiation of cat patients with nasal carcinoma. This system has proven to cope with the extremely high dose rate for MRT irradiations. We propose to further pursue the development of an on-line high resolution detector in MRT, which will allow the readout of peak and valley doses during the treatment and can be later integrated in a Patient Safety System, suitable for clinical trials.
The experimental dosimetry in MRT has made important progress over the last years, with a protocol for absolute dose measurements in place (12). High resolution dosimetry in MRT is still not perfectly matching the pre-calculated Monte Carlo dose calculations (13). Therefore, we propose to further improve these calculations by including diffraction and reflection effects of the MSC for more precise modelling. These improved calculations shall be benchmarked using adequate detectors like Gafchromic film, diamond detectors and other high resolution dosimeters.
Over the last 20 years the dose in the target for microbeam dose delivery has been determined by Monte Carlo calculations. Recently, S. Bartzsch has introduced some hybrid dose algorithm that has the advantage to be fast enough for patient dose calculations while remaining as precise as full MC calculations despite the small voxel sizes and the relative low energy photons. We plan to implement this hybrid algorithm into the research version of Varian’s Eclipse, a Treatment Planning System (TPS) platform for dose calculations in the clinical environment. This new dose calculation tool allows importing CT data from conventional scanners and shall be carefully benchmarked using an anthropomorphic phantom including high resolution valley dose measurements in the bone structures.
References
- Kahane P. [Epilepsy surgery in adult patients: for whom?]. Revue neurologique 2004;160 Spec No 1:5s179-184.
- Régis J, Rey M, Bartolomei F, et al. Gamma knife surgery in mesial temporal lobe epilepsy: a prospective multicenter study. Epilepsia 2004;45(5):504-515.
- Romanelli P, Fardone E, Battaglia G, et al. Synchrotron-generated microbeam sensorimotor cortex transections induce seizure control without disruption of neurological functions. PloS one 2013;8(1):e53549.
- St George EJ, Plowman PN. Surgery for temporal-lobe epilepsy. The New England journal of medicine 2002;346(4):292-295.
- Rheims S, Didelot A, Guenot M, et al. Subcontinuous epileptiform activity after failed hippocampal radiosurgery. Epilepsia 2011;52(8):1425-1429.
- Mori Y, Kondziolka D, Balzer J, et al. Effects of stereotactic radiosurgery on an animal model of hippocampal epilepsy. Neurosurgery 2000;46(1):157-168.
- Depaulis A, David O, Charpier S. The genetic absence epilepsy rat from Strasbourg as a model to decipher the neuronal and network mechanisms of generalized idiopathic epilepsies. Journal of neuroscience methods 2016;260:159-174.
- Pouyatos B, Nemoz C, Chabrol T, et al. Synchrotron X-ray microtransections: a non invasive approach for epileptic seizures arising from eloquent cortical areas. Scientific Reports 2016;6:27250.
- Pouyatos B, Serduc R, Chipaux M, et al. Synchrotron X-ray interlaced microbeams suppress paroxysmal oscillations in neuronal networks initiating generalized epilepsy. Neurobiology of Disease 2013;51:152-160.
- Bragin A, Engel J, Wilson CL, et al. Hippocampal and entorhinal cortex high‐frequency oscillations (100–500 Hz) in human epileptic brain and in kainic acid‐treated rats with chronic seizures. Epilepsia 1999;40(2):127-137.
- Chevassus-Au-Louis N, Ben-Ari Y, Vergnes M. Decreased seizure threshold and more rapid rate of kindling in rats with cortical malformation induced by prenatal treatment with methylazoxymethanol. Brain research 1998;812(1-2):252-255.
- Fournier P, Cornelius I, Donzelli M, et al. X-Tream quality assurance in synchrotron X-ray microbeam radiation therapy. Journal of synchrotron radiation 2016;23(Pt 5):1180-1190.
- Brauer-Krisch E, Adam JF, Alagoz E, et al. Medical physics aspects of the synchrotron radiation therapies: Microbeam radiation therapy (MRT) and synchrotron stereotactic radiotherapy (SSRT). Physica medica : PM : an international journal devoted to the applications of physics to medicine and biology : official journal of the Italian Association of Biomedical Physics (AIFB) 2015;31(6):568-583.
- Share
- Share on Facebook
- Share on Twitter
- Share on LinkedIn
- Share url